How Eyes Dominate Blended Vision
By: Anthony Vanrachack, OD
What is the difference between “blended vision” and “monovision”?
When I educate patients and student doctors about blended vision, there are many questions that come up, such as, Blended vision…what is the difference between “blended vision” and “monovision”? Aren’t they the same thing? “Old-school monovision” is when one eye is strictly far and the other strictly near. Vision zones are set so far apart that the brain may struggle to cooperate. On the other hand, blended vision zones overlap, so that the eyes work together with one eye far/middle and the other middle/near.
Some suggest: I’m right-handed, so I must be right eye dominant, right? I’ve found that you would be correct only about 75% of the time.
Well then how do you know which eye is the dominant eye?
Simply asking the patient which eye they shoot with could result in being incorrect 25% of the time.
If I catch a patient off guard, I’ll ask them to create a telescope with their hands and look at me through it. They may automatically wink their presumed non-dominant eye, looking through their cupped hands through their presumed dominant eye. Sounds easy enough right? Until they start looking through their handmade telescope to figure out why you even asked them to do that in the first place.
Other ways include having patients make a triangular pattern with their hands and look at a distant target as they bring the opening closer to their face. Their line of sight will be in front of their dominant eye. This can also be tested with a hole in a piece of paper and looking at an object of interest.
After binocular balance, I like to check for neuro/ocular dominance using the “retinoscopy lens” in the phoropter (the “R” on the auxiliary lens = +1.50). Keeping both eyes open, I alternate which eye has the retinoscopy lens in front of it. With this approach, the eye without the retinoscopy lens in front of it is the dominant eye.
Can a patient change their dominant eye? Yes! Below you’ll find a case where a patient successfully switched eye dominance.
What we found in a recent case.
We recently saw a 67 year old Hispanic female come in the clinic. She had a history of monovision OD far and OS near. See the details of her visit below.
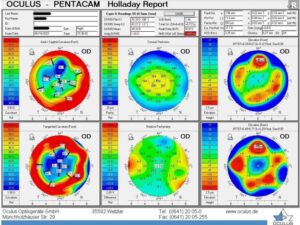
OD
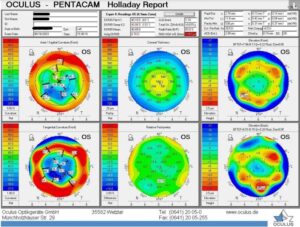
OS
- s/p RK OU
Slit lamp findings: 8 cut RK OD / 6 cut OS
4+ NS, 4+ PSC OD / 2+ NS, 1+ PSC OS
Serial topography demonstrated 1D change in Ks from AM to PM
Average Keratometry: OD flatter than OS
Cataract surgery OU (complex OD) performed successfully (two days apart, OD first, OS second).
LAL lenses were implanted with the initial intention to aim OD far, OS near.
Post-operative refraction ~1 month later demonstrated better vision potential OS compared to OD. Suggested switching dominant eyes.
1st LAL treatment performed OS first w/ plano target.
LAL treatments performed OD followed w/ -2.00 target.
Final MRx -2.50 OD, plano OS prior to lock-in.

A patient with a history of 32 cut radial keratotomy.
With proper education and reassurance, patients may be able to undergo different stages of neuroadaptation, those being conflict, tolerance, and acceptance. During the conflict stage, a patient may feel their eyes are working against each other, due to the brain wanting to see binocularly. The tolerant phase is when their brain starts to understand the eyes are doing different things, leading to summation or acceptance where both eyes open see better distance and near than monocularly. Once fully neuroadapted, many who undergo a procedure with blended vision targets feel so normal they are unable to tell you which eye is doing what until they cover their eye!
There are instances where a patient can switch ocular dominance and successfully neuroadapt, especially in the case where the previously thought non-dominant eye has the better vision potential. This is common where a patient may have an asymmetrical cataract and they feel their weaker eye has become the stronger seeing eye or in this case where a patient had a larger amount of radial keratotomy incisions in one eye than the other.
